
This is the final post in an eight part series on the history of Ebola. For immediate information about how to help prevent the further spread of Ebola and keep yourself safe please consult and share the Ebola Facts website.
As we are well aware, this year the two-decade trend of isolated outbreaks in Central Africa every few years has been broken by a much larger and more prolonged series of cases in West Africa. The outbreak began when a two-year-old child in southeastern Guinea contracted the most deadly species of the virus (Zaire ebolavirus) in early December last year, putting into motion the initially slow and then progressively faster spread of the virus to Liberia, Sierra Leone, and now Nigeria. Unlike the past twenty year’s string of Central African outbreaks that were each unique and separate despite initial speculation otherwise, this year’s West African outbreak does seem to be the result of a single index case followed by human-to-human transmission. Here’s a good time-lapse map of that transmission through West Africa. Summaries of the specifics of this year’s outbreak are widely available online, so I won’t go into too much detail here, but I will offer a few pieces of analysis based on the history I’ve covered in the previous posts.
 Matt Ridley gets it all wrong for The Times
Matt Ridley gets it all wrong for The Times
First there’s a need to correct a couple of pieces of misinformation that continue to circulate with this year’s outbreak. A more minor error is that this is not in fact the first time that there has been a West African case of Ebola as many news outlets have reported. Previously a zoologist working in Cote d’Ivoire caught the Tai Forest species of the virus and then fully recovered in Switzerland. Second and more importantly, the virus has not been previously restrained to only rural, remote areas of Central Africa. As we’ve seen, two of the deadliest previous outbreaks occurred when the virus struck the relatively large cities and regional hubs of Kikwit and Gulu. These Central African cities might not have quite the same level of road infrastructure linking them to other urban centers as West African cities do (although I know plenty of people board buses every day in Gulu bound for several cities and countries), but these two cases do provide a precedent for urban outbreaks of Ebola. And although these previous urban outbreaks were incredibly deadly, the cities were able to eventually contain the virus’s spread within a matter of months. So, in searching for a reason why this year’s outbreak has spread so far and killed so many, the answer is not as simple as stating that this is the first time the virus has appeared in an urbanized setting.
Other explanations have included the slow recognition and response time of international medical teams. Again, a look at the history of the virus shows that response time is not a unique factor in considering why this outbreak is so much worse. In the cases of the 1976 Sudan and Zaire outbreaks and several subsequent episodes, international teams were slow to recognize the virus’s appearance and did not arrive on the scene until after the local communities had already contained the spread of the virus. This fact suggests that one reason for the extent and deadliness of this year’s outbreak might be partly found in the local community’s responses. As Hewlett observed in Gulu, the DRC, and Gabon, many communities in Central Africa possess long practiced social procedures such as quarantine and modified burial practices that they employ when their communities recognize that they are dealing with an especially virulent affliction. I do not know if communities in West Africa have similar procedures, but it would not be surprising if they don’t due to the fact that they’re not used to seeing diseases like Ebola, or alternatively that they did previously possess similar response techniques but that the long civil wars in Liberia and Sierra Leone destroyed that local knowledge as violence and insecurity ripped communities apart.
Whatever the cause(s) behind the severity of this year’s outbreak, the fact is Zaire ebolavirus’s path through West Africa has been more deadly than all previous Ebola cases combined, and I have to admit that when I initially heard that the virus had arrived in Lagos—the impetus for this series of posts—I feared that Ebola might finally find in the fast life, international networks, and rancid infrastructure of Sub-Saharan Africa’s largest city what HIV/AIDS found in the reused medical needles, sex trade, and migrant networks of 1970s Kinshasa and Brazzaville—that is, the lethal mixture of social and environmental conditions that would allow the virus to eventually explode into a global epidemic.

Trash disposal in Lagos (Mark Duerksen 2014)
Being a Central African originating RNA virus linked to primates and transmitted through body fluids, comparisons of Ebola to HIV/AIDS were bound to occur. However there are several important differences that will likely yet prevent Ebola from boiling into an epidemic the way HIV/AIDS did. The first significant difference is the length of time from infection to fatality (or recovery for 10-60% of Ebola patients). HIV can hole up and multiply inside an infected person’s immune system for months, years, or even a decade, slowly destroying T-cells until it has killed so many that doctors consider the person to have developed AIDS. Over these months or years while HIV festers into AIDS, a person with HIV may be completely asymptomatic, but all the while still able spread the virus through sexual contact or blood transfusions. This slow and silent development timeline means that an HIV carrier might not even realize that he or she has become infected for years or even a decade and all the while be transmitting the virus to numerous people, allowing HIV to creep into a critical mass of carriers before it is even detected. This quiet buildup of an infected mass of people is exactly what happened for decades in Central Africa, and by the time doctors “discovered” HIV/AIDS, it was already an epidemic throughout the region.
Ebola on the other hand asymptomatically incubates for a few days or up to a few weeks, during which time the victim cannot transmit the virus to another person. Once symptoms develop after the incubation period, the patient’s health declines quickly and death is then generally a matter of days away, leaving only a very small window to further spread the virus (although it can still be contracted from infected corpses, so that is an additional concern and why burial practices are crucial to containing Ebola). One important note here is that those who recover from Ebola can still transmit the virus through semen or possibly breast milk for a number of weeks. While Ebola is easier to transmit during its small contagious window than HIV/AIDS is during its prolonged window, Ebola still has a low transmission rate,[1] requiring direct contact with infected bodily fluids, and the virus cannot be transmitted through the air the way respiratory diseases can be. Despite the horrific extent and fatality numbers of Ebola in West Africa, the virus will likely burn itself out due to its short contagious window (although it might take severe quarantine and curfew measures as we’re now seeing in West Africa) before it ever reaches a critical, completely uncontrollable mass in the way HIV did.
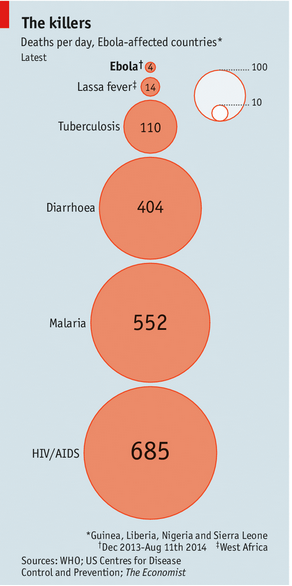
Perhaps the most optimism-inspiring difference between HIV/AIDS and Ebola is the two viruses’ rates of mutation. While both likely simmered in the forests of Central Africa long before scientists officially detected and classified them, Ebola’s genetic structure has hardly changed since the first confirmed cases in 1976 while HIV/AIDS has mutated incredibly rapidly, making treatment for HIV/AIDS much more difficult to square with virus’s continually changing configuration. Ebola’s steady genetic structure makes the prospects for a cure much more promising, and as we’ve seen with the initial success of ZMapp, cures seem to be on the horizon. Now we just have to hope treatments can be produced and distributed asap because, while Ebola is not likely to become a global epidemic, it is causing untold suffering in West Africa that we likely won’t realize the true extent of for some time yet. Ebola’s destructive path through West Africa includes not only the direct victims of the virus, but also those caught in the clashes between soldiers enforcing quarantines and those trying to flee its path, survivors who are now shunned by their communities, communities that no longer trust doctors and hospitals, businesses and entire economies that have taken a massive hit, and medical infrastructure throughout the region that has been depleted, abandoned, and looted, causing other illnesses to proliferate in the absence of treatment facilities. Still it is worth noting the statistics on HIV/AIDS and other deadly diseases deaths per day dwarf Ebola deaths in the Ebola-affected countries–a reminder that those preventable diseases also require immediate attention and that serious long term work to repair medical infrastructure and communities’ relations with medical personnel will be imperative to West Africans’ health once this outbreak can be contained.
[1] Daniel G Bausch, et al., “Assessment of the Risk of Ebola Virus Transmission from Bodily Fluids and Fomites,” Journal of Infectious Disease, 196(), S142-S147. Available online: http://jid.oxfordjournals.org/content/196/Supplement_2/S142.full

Update: great article on how Nigeria has managed to successfully contain Ebola: http://www.pbs.org/newshour/bb/nigeria-succeeded-containing-ebola/